
CBS News Builds Measles Fear While Ignoring Vaccine Injured Woman in Clark County
In late 2023, Stephen Stock of CBS visited Clark County to resurrect the history of the 2019 measles outbreak and interview stakeholders involved during that time, from Clark County Local Health Officer Alan Melnick to an immune-compromised family. Many ICWA members, supporters and followers were very involved during the 2019 events and are painfully aware of the many details to the story.
As we reported on December 27, they also interviewed Misty Gehrke who, at the advice of the health department, took a booster MMR shot ‘just in case.’ Her interview has not yet aired.
In summary:
- CBS News recently released many reports like “Thousands of school-aged children are at risk of getting sick from measles, and “Data shows at least 8,500 U.S. schools at greater risk of measles outbreaks as vaccination rates decline.”
- Common fear tactics were utilized:
- Tactic 1: False vaccination rates – quoting data from an optional, under-utilized database, Washington’s Immunization Information System (WA IIS), rather than the required-by-law school reports.

CCPH 2018 MMR Rates of 78 percent per IIS was last posted on April 17, 2020. This post is no longer available. Meanwhile, the school reports show Clark County as having 85% of Kindergartners complete for MMR, and this number goes up as paperwork is completed and as kids complete the age range for the booster dose.
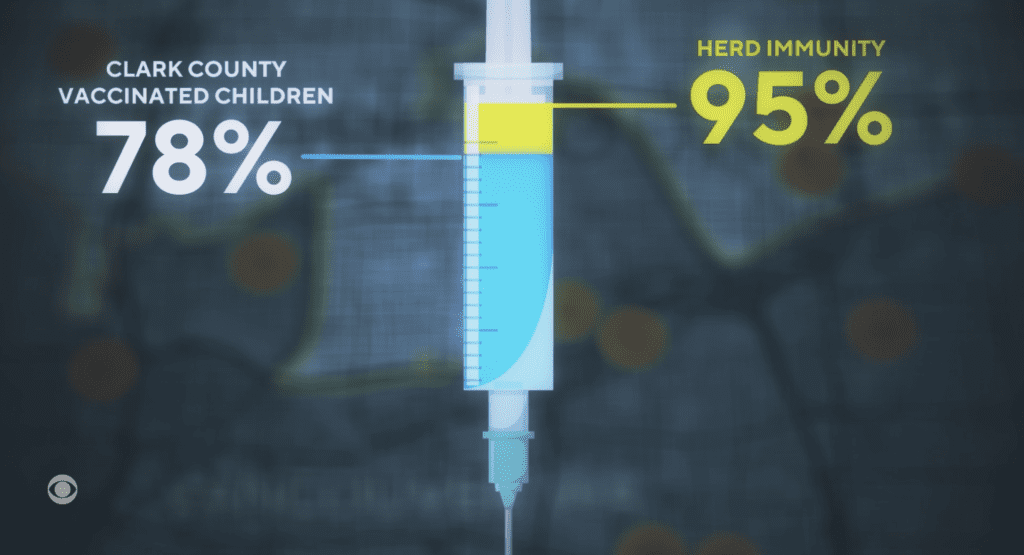
- Tactic 2: Stating that low rates led to a lack of “herd immunity” and rapid spread – however, infections spread because of intentional susceptibility in a smaller ethnic community among families with many children, and who self-isolated, greatly lowering any risk to the immune compromised.
The CDC’s own report says: “Households and churches were the predominant settings for transmission, associated with 36 (51%) and 18 (25%) of the 71 patients, respectively . . . Among the 30 patients identified after February 1, 26 (87%) were known contacts in quarantine and under active surveillance, decreasing public exposures by implementing effective social distancing strategies.”
- Tactic 3: Raising alarm that a child undergoing immune-compromising medical treatment will die if everyone else doesn’t get vaccinated. While it’s true that measles is potentially more serious and life-threatening to those with severely compromised immune system, such individuals are also at risk from many viral infections and unlikely to be attending school or other public places during outbreaks, no matter the community vaccination rate.
- Tactic 1: False vaccination rates – quoting data from an optional, under-utilized database, Washington’s Immunization Information System (WA IIS), rather than the required-by-law school reports.
- Common fear tactics were utilized:
- Clark County resident Misty Gehrke was permanently disabled in 2019 by an MMR vaccine. Although CBS interviewed her, they did not include her in any report yet. See our initial story.
- CBS also conspicuously left out the group interview of Misty, ICWA Director Bob Runnells, the former president of the Family Freedom Coalition Janna Meyer, and ICWA data researcher Karl Kanthak.
- Karl Kanthak provides analysis of the 2019 House Bill 1638 that removed the personal exemption to the MMR, showing it did not increase vaccination rates, but instead drove up religious exemptions and drove families out of the school system.
- To-date, 111,945 adverse events have been reported to VAERS (Vaccine Adverse Event Reporting System) for any measles-targeting vaccine. These data must take into account the underreporting inherent in this passive reporting system, where a 2011 CDC study found that “fewer than 1% of vaccine adverse events are reported.” Thus, the actual injuries must be more common than ‘rare.’
Let’s breakdown the video featured in many of the CBS National News articles that are available for local CBS affiliates to monetize the fear in their broadcast markets.
In an obvious attempt to dramatize the non-emergency, the CBS video starts with footage of a school bus in the rain, a mother leading her child onto the school grounds, with a mother saying: “It started out like any other normal year.”
CBS then showed footage of children being led to Minnehaha Elementary School in Vancouver, Washington under dreary skies.
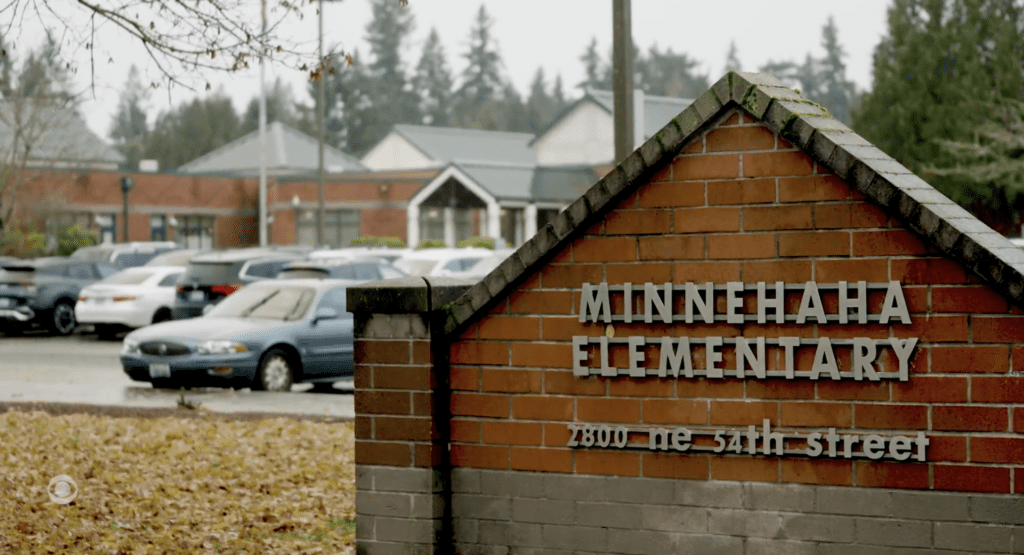
When the school’s sign is shown, CBS had a broadcaster saying, “Also, today, a new exposure site. We’re told a non-student and non-staffer went there while contagious.” It’s not clear if he meant that is today’s news, or if he’s going back in time to dramatize the case-zero moment. Either way, that elementary school was not involved in the earliest cases, so any immune-compromised students had plenty of warning to avoid public places. With approximately three news articles per day in the local newspapers, there was plenty of warning.
Clark County Public Health Officer Dr. Alan Melnick is thrust into view: “We knew that it was going to be a crisis.” The report quickly switched to science teacher William Baur at his desk: “It was a matter of time that our school was going to have a case,” he said.
Switching quickly again, CBS Reporter Stephen Stock then asked mother Jessica Fichtel, “Were you scared?” She replied, “Terribly. Terrified.”
With another shot of school buses in the rain, a broadcaster’s voice is heard: “The Pacific Northwest is becoming a hotspot for both children suffering from measles and parents who do not want to vaccinate their children.”
The next overhead voice comes from CBS Reporter Stephen Stock: “Clark County, Washington, made national news in 2019 with a measles outbreak that lasted for months.”
Next came a quick succession of quotes in between Stock’s narrative, starting with the controversial Dr. Melnick, who has been relieved of his public health officer duties in two other Southwest Washington jurisdictions: Lewis County in 2022 and just recently, Cowlitz County.
- Dr. Alan Melnick: It was kind of something waiting to happen.
- Stock’s narrative: It started with one case.
- Melnick: But you’re trying to work as quickly as you can and reach people.
- Stock’s narrative: Then came another and another.
- William Baur: Well, there was an exposure there, and so they called and let me know.”
- The fear tactics heightened when Stock focused his report on Jessica Fichtel and her son:
Stock’s overarching narrative: During the outbreak, Jessica Fichtel’s son battled childhood leukemia at just six years old
Jessica: I distinctly remember being terrified. His life would be in grave danger if he would have been exposed to measles and contracted it.
As CBS film editors showed the above needle with a map of Clark County in the background, Stock said, “In a matter of three months, the measles outbreak in Clark County had climbed to seventy-one cases. The rapid spread happened because the number of vaccinated children was well below the minimum level the Center’s for Disease Control says is needed to prevent an outbreak.”
We can remind readers that measles are infectious for up to 8 days. Therefore, there were no more than about 20 infectious cases at any one time in a county of nearly 500,000. The statistics did not match the panic in the media or in Mr. Stocks dramatization.
Stock also did not mention that all seventy-one safely recovered from the measles. Those seventy-one now have lifetime immunity, unlike the vaccinated who have inferior and less durable protection. But Stock never told the public those inconvenient details. Instead, they fanned fear that every person in the state was in danger of a “dread” disease.
CBS News then blamed the Clark County outbreak on its inability to reach herd immunity.
Dr. Matt Ferrari from Penn State added the following: “Herd immunity, simply put, is just the indirect protection to a non-vaccinated person of being surrounded by vaccinated people, right? Those vaccinated people act like a shield.”
Stock then narrated, “But in 2019, Clark County, Washington, didn’t have that shield.”
William Baur said, “I got an email from the principal that we’re having to shut down.”
Stock stepped in with more narration: “Schools here had to go to remote learning a year before COVID-19 closed classrooms everywhere. Science teacher William Baur says it all could have been avoided.”
“I would say that I felt angry,” Baur said. “Like I’m kind of frustrated that there is this vaccine skepticism.”
Stock then pointed to the Clark County story as part of a nationwide event: “Nationwide, the share of unvaccinated kindergartners grew significantly in the last three years. And in the nineteen states where we analyze the data, the vaccination rates are so low at least 8,595 schools across the country are at risk of a measles outbreak.”
In step with the anti-misinformation campaigns being performed by the Washington Department of Health (DOH), the University of Washington, and even as large as the World Economic Forum, CBS blamed the public for having misperceptions of the measles vaccines.
“The reason rates are down is complicated. Six different experts we talked with point to political influences, misinformation, mistrust in government, and fear of vaccines.”
Dr. Ashwin Vasan of New York City Public Health added the following: “We now have a misinformation superhighway, which is social media, and you can get pretty sophisticated in the ways that you target misinformation to certain communities.”
Stock then said that another factor was the nonmedical exemptions for religious or philosophical reasons. “The CDC reports that exemptions were up in forty-one states for the last school year,” he said.
Jessica Fichtel shook her head about people not taking the measles vaccines: “I just can’t wrap my head around why you wouldn’t do it,” she said.
The recent case of Clark County resident Misty Gehrke is good reason why someone would not want to take the vaccine.
Until early March 2019, Misty Gehrke was an early childhood educator in Clark County. Both of her seven-year-old twins had received childhood MMR shots, so she wasn’t worried about them or the so-called outbreak before she was called by the health department. She had read that state legislators proposed a bill requiring daycare workers to be up-to-date with their MMR shots.
Stephen Stock had interviewed Misty, but, as much as he focused on Jessica and her son, he never mentioned Misty’s permanent disability after receiving the measles shot. In the interview that has not yet been aired, Misty told Stock that she wasn’t concerned about getting the measles.
Misty did have her measles titers checked. The level was low and they said she should get the ‘booster’ if she wanted to return to work as soon as possible. Eighteen days later, she was paralyzed.
“So I called my mother, and she took me to the emergency room.” The neurologist diagnosed her with Guillain-Barré Syndrome (GBS), which is recognized on the injury table for the vaccine court established under the National Childhood Vaccine Injury Program.
While Misty was busy rehabilitating herself, the state legislature passed the bill that now requires child care workers to get the shot. The bill not only removed the personal exemption to the MMR vaccine for kids, but also enacted Washington’s first vaccine mandate for adults, requiring day care workers to show proof of MMR vaccination, proof of immunity, or a medical exemption. [RCW 43.216.690] This law for adults does not allow for religious or non-medical exemptions, while parents can claim a religious exemption from the shot for their kids.]
Back to the released CBS News report, Stock offered the following narration: “In Jessica’s world, the vaccination rate is trending down again.” Jessica then inserted, “It’s crazy,” before Stock went on to narrate, “Two-thirds of Washington state schools are now below the threshold for herd immunity. That’s 53,000 students at risk.”
The story then ended with Jessica saying, “Why wouldn’t you do it for the five-year-old who, if he were to get measles, he’s going to die.”
Besides leaving out his interview with Misty Gehrke, Stock also conspicuously left out his group interview that, besides Misty, included ICWA Director Bob Runnells and ICWA Data advocate Karl Kanthak.

CBS National News Reporter Stephen Stock interviews Misty Gehrke, along with Karl Kanthak (researcher), Bob Runnells (ICWA Director) and Janna Meyers, all who were parents of schoolchildren during The Great 2019 Clark County Measles Inbreak.
During the interview, Stock seemed so intrigued by Karl’s ability to refute the DOH’s and other agencies’ claims that the vaccination exemption rates are down that he asked him to e-mail him more information and links. “I like doing research,” Stock said during this interview.
In turn, Karl wrote the following to the CBS reporter.
Dear Mr. Stock,
It was good to meet you yesterday. I rarely encounter any media personnel with more than a superficial knowledge of vaccination issues beyond talking points.
To Clarify:
There is no dispute that Dr. Melnick did not use the official, school registration-based CIS data in January 2019.
Clark County Public Health department freely cited the inferior IIS as the source of the “78% rate”, before scrubbing it from their website and communications.
Here is a screen shot of the page.
There is no dispute that the IIS undermeasures by 15% or more. https://doh.wa.gov/sites/default/files/legacy/Documents/Pubs//348-565-ImmunizationDataTechnicalNotes.pdf
If Dr. Melnick is representing to you that the IIS “78% MMR” are school rates, he is intentionally misleading you. Dr. Melnick knows the IIS is the inferior system, and January 2019 is only time he has ever used IIS misrepresented as school rates, prior or since.
Dr. Melnick knows that the vast majority of people do not have any understanding that there are various different vaccination tracking systems and reports. He used that ignorance against his governing board to confuse them when I informed them of the actual CIS data.
Dr. Melnick is also abusing the inherent trust people have that as a Public Health Officer that he would only report the most accurate data and conduct himself in an ethical manner.
If Dr. Melnick does “fess up”, and admit to you that the IIS is not the actual school rates, his wiggle positions would be:
“We found that the IIS was more accurate”- that is impossible as I address in excruciating detail in my report, and the opposite of all tracking system comparisons performed by various state agencies and the technical note linked above.
Or
“We are not actually misrepresenting the school rates because the reference doesn’t say “students”, it only lists an age range of children”:
“As of Dec. 31, 2018, 78 percent of Clark County 6- to 18-year-olds have received two doses of MMR (measles-mumps-rubella) vaccine, which is the age-appropriate number of doses.”
That would be very sleazy, and is ridiculous, as Dr. Melnick frequently stated publicly it is the school rates.
This is also impossible as there are simply not enough home school students to dilute and drive the overall county school rates to 78%, even if none of them were vaccinated. The IIS is that bad.
If the problem actually were children who are not school students, why push legislation impacting school attendance exemption availability which would not address that issue anyway?
There is no point in restricting exemption accessibility when the rate is only 5.3%. If any of the 94.7% of not-exempt students aren’t vaccinated it is not because of exemptions, it is another cause and exemption legislation is mis-directed.
So, you have a story here, but it is probably not the one you expected.
A county health officer, in coordination and cooperation with his county agency, and the State Department of Health including the state Secretary of Health, fraudulently misreported the material facts of how many Clark County K-12 students received MMR injections and used exemptions.
They made this misrepresentation to the Clark County Council and CC Public Health Board, the WA State Board of Health, Clark County officials, the WA State Governor’s Office, the WA state legislature, WA State Federal Congressman and Senators, the Federal Senate and Congress in hearings, and the media and the public.
The only logical reason to use the wrong data being to alarm the electorate into passing exemption restricting legislation.
In Dr. Melnick’s “defense”, his misrepresentation of basic facts is common and typical for every county and state health department I have interacted with. This is detailed at https://karlkanthak.substack.com/p/introductory-videos. There are 2, 3-minute introductory videos there to give an overview.
Outbreak
You asked how Clark County could have an outbreak if the exemption rate is only 5.4% and the vaccination rates are above 93%?
The reason that 93% plus vaccinated Clark County had an outbreak is because a child introduced measles from Ukraine into a religiously exempt, intentionally unvaccinated, insular Slavic religious group during the Christmas and New Year celebration season where there were full group pageants, other congregations and family gatherings during the timing when the initial infection seeding took place.
The resulting first outbreak cluster in mid-January was from those holiday church and family exposures, then a second cluster from the private Slavic school, Bible Study, Sunday school and Russian school exposures in early January. The Slavs actually closed for a couple of weeks. February 1 forward cases were already in surveillance, meaning they were family / contact of cases.
76% – 54 of 71- cases were home and church transmissions, leaving only 17 for school, daycare and “unknown”. The case timing in the CDC report describes the seeding church / home events, then Slavic school exposures, then family member transmission in home scenarios. https://www.cdc.gov/mmwr/volumes/68/wr/mm6819a5.htm
The Slav’s seemed to think they were the only cases from their interactions with public health, and they reached out to the media, and the Pastor wrote an “open letter”, to try to calm things down and reassure the larger public they were at low risk.
From a logistical standpoint, there are only 4,000 MMR exempt students spread out over 186 schools in the Clark County population of 500,000, in a physical area over 600 square miles.
What is the chance of random encounters between unvaccinated children being in the same public place? There is significant evidence pointing to the majority of cases being centered in this community.
How does a county drop to a 78% MMR rate “out of nowhere?”
During the outbreak and subsequent legislative push, I notified the Clark County Council, which is also the Clark County Board of Health, of this misuse of data.
At one Health Board meeting I explained that it takes 13 years to establish a vaccination rate in a K-12 system.
If the Senior Class of 2019 has an only “77% MMR” rate, then 13 years ago when they entered kindergarten it would have to have been only “77% MMR” then, and never increased for the following 12 years.
And every new Kindergarten class after 2006 would also have to be at “77% MMR”. Where was Dr. Melnick over those years?
I spoke privately with council members who were very confused by this sudden crisis in the vaccination rates, as they receive an annual briefing, and never before, (and never since the end of the 2019 legislative session), did Dr. Melnick report either low vaccination rates or excessive exemption use.
How did this vaccination deficiency build itself up to a point where “suddenly” the entire K-12 system is at only “78%”?
Council member:
“How did Clark County “suddenly” go from “everything is fine except rates can always be higher”, to “our rates are so low we cannot stop outbreaks?””
“If we are really at 78% MMR, it is Dr. Melnick’s fault because we were never told there was a problem and isn’t it his job to be monitoring this?”
When they understood that Dr. Melnick intentionally pulled data from a system other than the CIS, they confided to me,
“What can we do? He is the top employee in the department and telling us something we don’t think is correct. If we ask any questions we get labeled “anti-vaccine”.”
I hope you are able to review the material I left with you, and I am happy to provide any clarifications, discuss, or provide feedback.
I have unintentionally become a subject matter expert on school vaccination policy, its intersection with education policy, and legislation.
Additional resources
My analysis of EHB 1638 and the new misrepresentations is here https://karlkanthak.substack.com/p/school-exemption-advocate-alert
I am including slides from a National Vaccine Advisory Committee meeting detailing that the CA DPH considers protection from the MMR to be tenuous, so they direct their personnel to consider themselves susceptible to measles regardless of vaccination status when treating measles cases. If MMR cannot reliably protect a Health Care Provider from infection, can we expect it to do so for any other vaccine recipient?
Best Regards,
Karl Kanthak
Besides the case of Misty Gehrke, Stock conspicuously did not share with his viewers the adverse events following measles vaccinations reported to VAERS, which shows 111,945 cases of adverse events reported in the United States and its territories.
Furthermore, it is important to note that the Vaccine Adverse Event Reporting System (VAERS) is a passive, voluntary system, jointly managed by the CDC and FDA, that accepts reports from anyone. A 2010 HHS study of the government’s notoriously dysfunctional VAERS concluded that VAERS detects “fewer than 1 percent of vaccine injuries.”
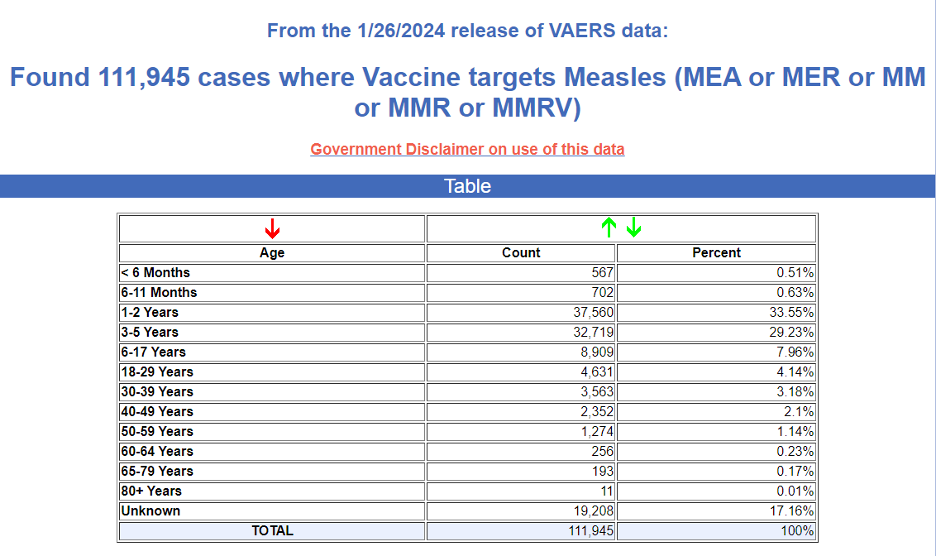
Of those adverse events, 556 resulted in death.
In Washington, VAERS shows 2,515 adverse events following measles vaccinations.
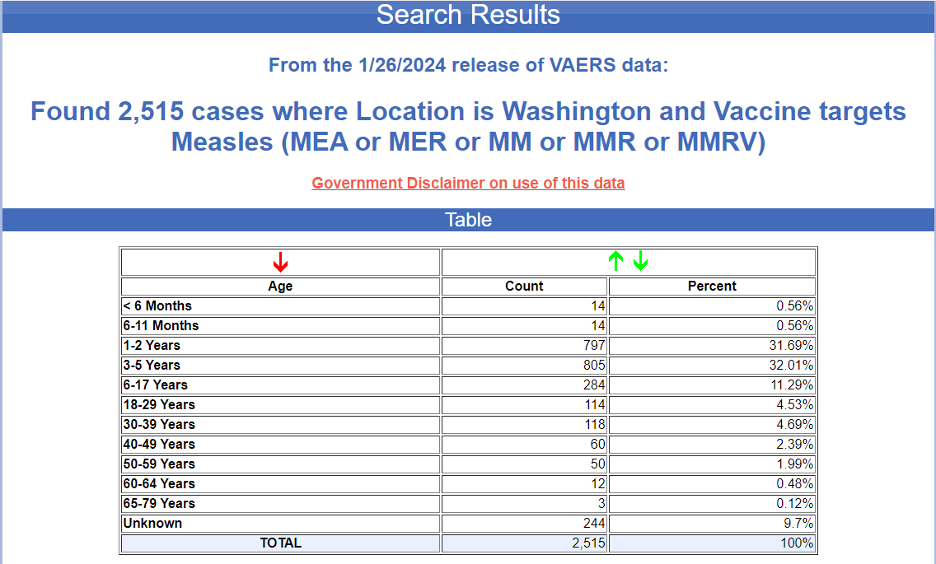
Four of those adverse events resulted in death. They are as follows;
| VAERS ID: | 56638 |
Submitted write-up: deep sleep/unconcious, t102.8, adm to hosp cerebral edema, papilledema/infarctions, brain death/cardio resp failure;
| VAERS ID: | 338821 |
Submitted write-up: This case was reported by a healthcare professional and described the occurrence of death nos in a 12-month-old female subject who was vaccinated with HAVRIX (GlaxoSmithKline), MMR II (strain not specified), VARIVAX and PREVNAR. On 21 January 2009 at 07:43, the subject received unspecified dose of HAVRIX (.5 ml, unknown, right thigh), unspecified dose of MMR II (unknown), unspecified dose of VARIVAX (unknown), and unspecified dose of PREVNAR (unknown). On 22 January 2009, 1 day after vaccination with HAVRIX, after vaccination with MMR II, PREVNAR, and VARIVAX, the subject experienced death nos. The healthcare professional considered the event was disabling, life threatening and clinically significant (or requiring intervention). The subject died on 22 January 2009 from death nos. It was unknown whether an autopsy was performed. It was reported the subject had “no history of illness or medical problems. Not on medications at time of death. Medical examiner stated undetermined cause of death on death certificate”. 3/5/09 Autopsy report received with COD: Undetermined. Manner of Death: Undetermined. Child had presented to PCP earlier on the DOD with fever and URI sx. 4 vax given taht day. Child remained cranky and put down to nap. Approx 1 hour later found face down without pulse or respirations. Resuscitation unsuccessful.
| VAERS ID: | 664201 |
Submitted write-up: Parents report intermittent illness since vaccination: fever(101) every other day x7 days, nausea, vomiting, diarrhea, headache, fatigue, somnolence, dizziness, cough, Left leg pain.
| VAERS ID: | 862890 |
Submitted write-up: Write-up: Patient is a previously healthy 13 month old boy who presented with respiratory failure, then developed ARDS and multiorgan dysfunction on VA ECMO, requiring vasoactive support and CRRT. Subsequently found to have multiple disseminated viral infections, including HSV, adenovirus, and low level positive CMV and EBV. Suspected immunodeficiency, workup pending. In setting of recent MMR and varicella vaccinations, critical illness, and suspected immunodeficiency, workup for disseminated vaccine strain measles sent at CDC. Positive for vaccine-strain measles from nasopharynx and urine. Patient initially presented with an otitis media on 1/30 and then re-presented with stridor and rapid respiratory failure. Evidence of epiglottic inflammation with “white dots” noted during intubation and cervical & retropharyngeal lymphadenitis. He had a respiratory PCR positive for adenovirus and RSV and serum positive for adenovirus, though not remarkably high level. EBV PCR in serum also low-level positive but serology from OSH suggestive of past infection. I&D of L neck lymphadenitis performed; cultures from lymph node I&D are negative. CT with evidence of developing retropharyngeal phlegmon. Subsequently developed knee lesion which was positive for HSV, HSV PCR from serum shows disseminated HSV at high viral levels. EBV and CMV positive at low levels, also HHV6 positive, likely represent reactivation in setting of severe illness. Based on multiple viral infections, immunology team involved and on DDX are immunodeficiencies such as TLR defects. HLH/MAS was considered and he met some criteria for this; was on anakinra and received intermittent steroid dosing. BAL cytology from 2/14 showed multinucleated giant cells. ETT quantitative RSV level pending. When measles results from NP/urine returned on 2/21, started on oral ribavirin (while pursuing IV ribavirin), high dose vitamin A, and redosed IVIG. HSV level continuing to fall. Unclear of contribution of measles vaccine strain to respiratory presentation; felt to be unclear whether represented prolonged shedding versus true pneumonia/pneumonitis. Further testing at CDC pending including measles IgM and measles PCR on deep respiratory sample.