
Lies, misrepresentations, and misleading data
by Dr. Carver
First published Feb. 16, 2022 on Dr. Carver’s sub-stack Zana’s Newsletter. Republished with permission.
Washington State Department of Health is meeting this Thursday and next Thursday to discuss adding the COVID-19 experimental products to the vaccine schedule for children to attend school and day care. They are being advised by a Technical Advisory Group (TAG) evaluating 9 criteria. I will be responding only to criteria 5 in this post.
General Issues
The experimental COVID-19 injections are not classical vaccinations in which antigens are provided to the body in order to stimulate an immune response. The pediatric Pfizer injection is a mRNA technology inside a lipid nanoparticle carrier, which causes gene expression of the antigen in vivo. The expressed antigen is the S1 subunit of the spike glycoprotein.
The S1 antigen that the mRNA product causes the body to produce is based on an in-silico model of the original alpha strain of the spike glycoprotein of SARS-CoV-2. Since the emergence of the alpha strain, there have been many variants with slightly different morphological features. The Omicron variant has displayed a significant morphologic divergence from the original alpha strain as evidence by the decreasing effectiveness of these inoculations towards different variants (95% effective against the alpha/wild type strain, 39-42% effective against Delta, and an inverse efficacy against Omicron -meaning infection is more likely with a greater numbers of boosters).
“Original Antigenic Sin: Those who are infected with pathogens for which the vaccine is an insufficient match make up another portion of those who remain at risk of infection.”
This creates selective pressure for viruses to evolve in a way that makes them more transmissible within the vaccinated population.
It needs to be acknowledged how the goal post with these experimental products has changed. First, they should have tested if these injections reduce infection rates with an absolute risk reduction calculation. Others have calculated the absolute risk reduction to be less than 1%. Second, when they couldn’t fool the public with their relative risk reduction calculation, they moved the endpoint to measuring a difference in severe COVID morbidity and mortality. However, this was never accurately assessed since in Pfizer’s own pivotal trials the effect size was too small to measure this endpoint and with studies in children, there was no proper control group. They used an immuno-bridging procedure that uses a control group from another age category and for anyone who understands the scientific method, this is grossly inadequate. In addition, the controls were unblinded in the original pivotal trial so no one can in good faith refer to a double blind controlled clinical trial. Lastly, the statistical methods were inadequate, namely the lop-sided data exclusions that overwhelm the effect size. When the pivotal trial data was re-analyzed, it showed a large increase in overall mortality in the vaccinated treatment group.
The experimental injections cause antigens to be produced in the wrong compartment of the body. In a natural infection the innate immune response of the mucosal membranes is stimulated resulting in immunological memory that is broad, robust, and durable. A natural infection involves memory cells of both cellular and humoral origin which leads to a faster, more efficient, and longer duration immune response on re-exposure to the same or similar pathogen. Not only is this natural process broad and highly integrated but it protects the mucosal membrane borders of the body, with secretory IgA. In contrast, the mRNA product causes the antigen to be produced in the deltoid muscle and systemically throughout the cardiovascular and lymphatic systems. This means that the mucous membranes are not protected from the virus because the antibodies (IgG and IgA) are produced systemically (in the blood rather than in externally bordering tissues of the body.) This means it’s highly unlikely the mRNA given intramuscularly could ever prevent infection.
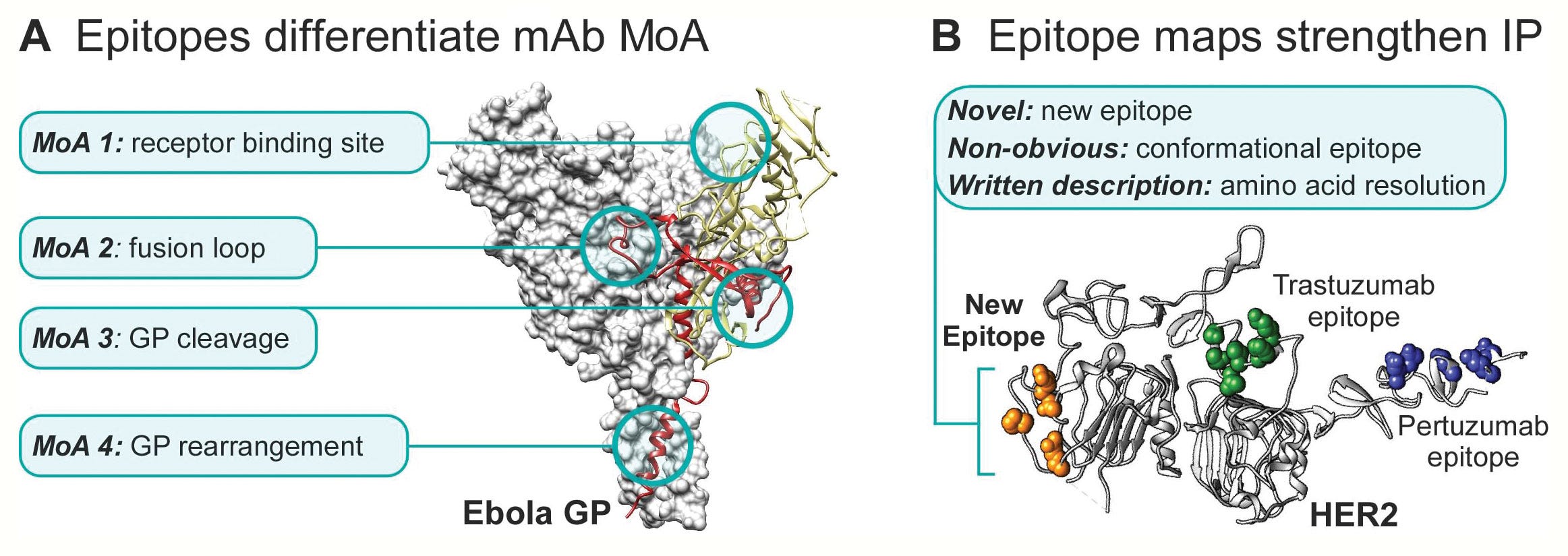
In addition, a natural immune response is polyclonal (1000’s of antibodies with different receptors are produced.) This is much different than the targeted immune response to a subsection of the spike protein as in artificial immunity. To put this another way, in a natural immune response, the antibodies target all the virus in a multitude of ways, including the nucleocapsid portion. That means when there is another variant some of those antibodies will be cross reactive and effective against the new variant. This cannot be stated with the targeted and limited artificial mRNA approach to a portion of the spike protein only.
Below is an image showing multiple areas for different antibodies to bind to an Ebola epitope (antigenic determinant or piece of an antigen.)
There is evidence of secondary vaccine failure, where the levels of antibodies decrease over time requiring an endless stream of booster shoots. This completely ignores the fact that there is innate and T-cell memory that remains accurate and effective for those with robust natural immunity.
Mortality and Morbidity?
So now that we’ve established the so-called C-19 vaccines do not contain any antigen that prevents any disease, what about reducing mortality and morbidity? These endpoints have not been properly studied. One reason for this is conflating the terms “with COVID” vs. “from COVID” in relation to hospital admissions. The other reason is the change in terminology, for example, a COVID infection in a vaccinated person is now called “COVID pneumonia” and is not coded or counted as a COVID case. Furthermore, some hospital staff have been pressured to write “unknown” for vaccine status if a patient is vaccinated and has been admitted to the hospital for COVID.
I submitted a FOIA to our state department of health to find out the numbers of vaccinated and unvaccinated people admitted to the hospital for COVID. To my surprise, they do not have this information, only broad information on the percentage of people vaccinated and unvaccinated in each county and separate information on hospital admissions for COVID without vaccine status listed. THERE WAS NO ATTEMPT TO STUDY IF VACCINATED PEOPLE ARE MORE OR LESS LIKELY TO BE ADMITTED TO A HOSPITAL FOR COVID TREATEMENT! In summary we do not have evidence of vaccines reducing COVID morbidity or mortality but what we do have is ample evidence of the increase in overall mortality caused by the C-19 experimental injections.
Currently, there are 1,103,891 adverse events reported to the vaccine adverse events reporting system (VAERS) for COVID-19 injections alone. When considering that only a fraction of adverse events is reported (1% according to a Harvard study), the real numbers are certainly much higher. The VAERS reports are vetted by CDC staff before becoming publicly available. Of those adverse events, there have been 32,426 reports of myocarditis/pericarditis. There is no public access to the V-safe database and NO opportunity for independent scientists to access their data.
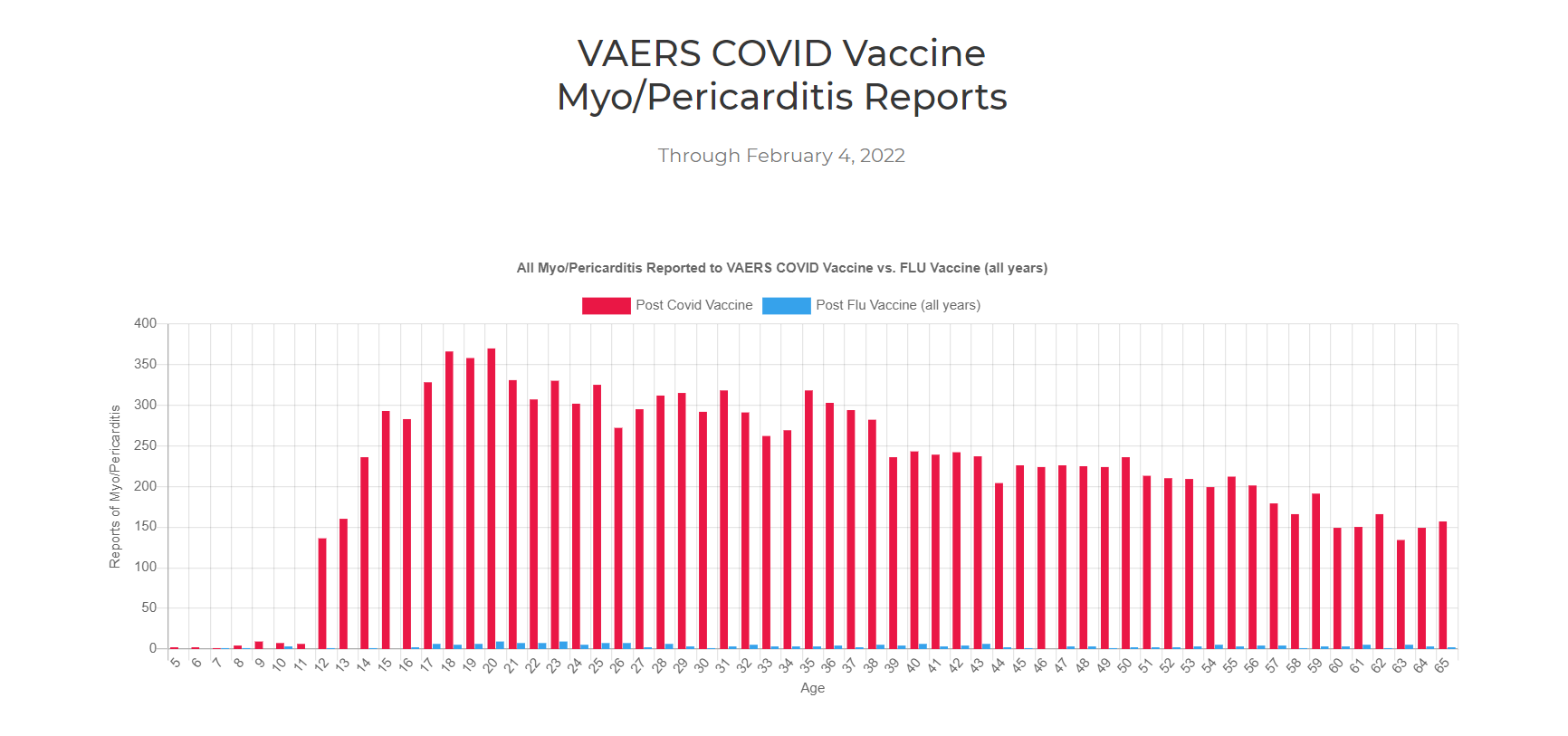
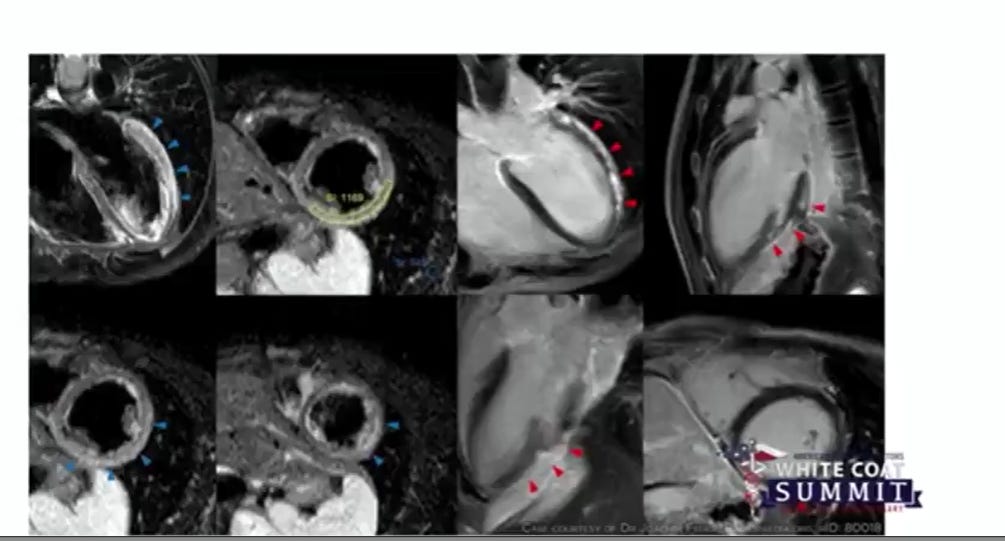

Images from OpenVAERS.com and White Coat Summit, Dr. Ryan Cole.
The VAERS reports are supported by recent data from the Defense Medical Epidemiological Database (DMED), in which it was found: below are summarized 2021 (+ vaccine) numbers % change relative to 2020 (- vaccine).
Total Number of Diseases & Injuries Reported by Year (Hospitalization) up 37%
Total Number of Diseases of the Nervous System by Year up 968%
Total Number of Malignant Neuroendocrine Tumor Reports by Year up 276%
Total Number of Acute Myocardial Infarct Reports by Year up 343%
Total Number of Acute Myocarditis Reports by Year up 184%
Total Number of Acute Pericarditis Reports by Year up 70%
Total Number of Pulmonary Embolism Reports by Year up 260%
Total Number of Congenital Malformations Reports by Year up 87%
Total Number of Nontraumatic Subarachnoid Hemorrhage Reports by Year up 227%
Total Number of Anxiety Reports by Year up 2,361%
Total Number of Suicide Reports by Year up 227%
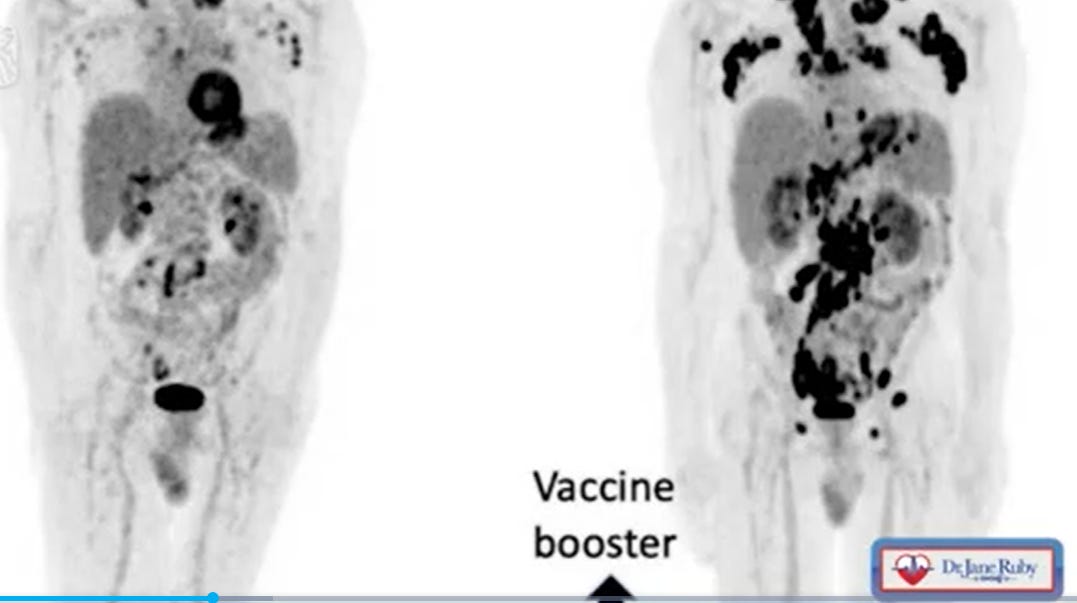
Total Number of Neoplasms for All Cancers by Year up 218%
Total Number of Malignant Neoplasms for Digestive Organs by Year up 477%
Total Number of Neoplasms for Breast Cancer by Year up 469%
Total Number of Neoplasms for Testicular Cancer by Year up 298%
Total Number of Female Infertility Reports by Year up 419%
Total Number of Dysmenorrhea Reports by Year up 221.5%
Total Number of Ovarian Dysfunction Reports by Year up 299%
Total Number of Spontaneous Abortion Reports by Year DOWN by 10%
Total Number of Male Infertility Reports by Year up 320%
Total Number of Guillain-Bare Syndrome Reports by Year up 520%
Total Number of Acute Transverse Myelitis Reports by Year up 494%
Total Number of Seizure Reports by Year up 298%
Total Number of Narcolepsy & Cataplexy Reports by Year up 352%
Total Number of Rhabdomyolysis by Year up 672%
Total Number of Multiple Sclerosis Reports by Year up 614%
Total Number of Migraine Reports by Year up 352%
Total Number of Blood Disorder Reports by Year up 204%
Total Number of Hypertension (High Blood Pressure) Reports by Year up 2,130%
Total Number of Cerebral Infarct Reports by Year up 294%
The increased cases of mortality in the vaccinated are corroborated by the One American Life Insurance Company. They found a 40% increase in mortality in those aged 18-64 that correlates perfectly to the vaccine rollout dates.
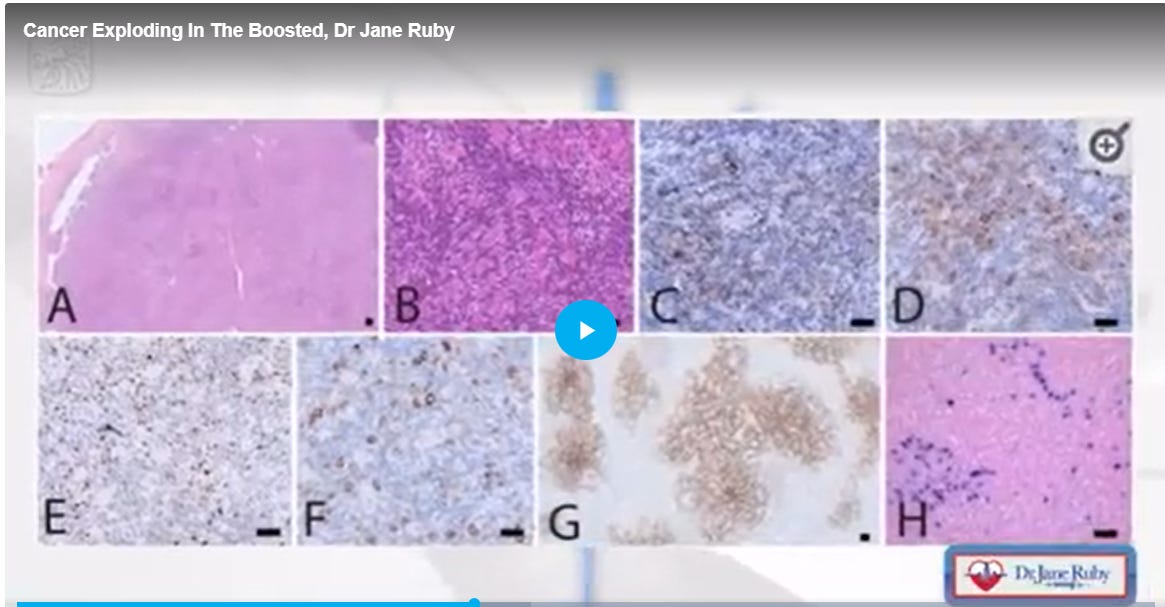
The increased cases of vaccine deaths have been confirmed by case studies, autopsies, post-mortem pathology results, and morticians worldwide. Embalmers, Mr. Hirschman, and others are seeing unusual clots in 50% to 93% patients with many of those patients confirmed as having been vaccinated.
A paper written by Dr. Bhakdi and Dr. Burkhardt examined the pathology of those who died after being vaccinated. They found that 93% of those deaths were caused by the COVID-19 vaccines even though the coroner did not implicate this on any of the death certificates.
How the Data Presented by the Technical Advisory Group (TAG) who advises the Washington State Board of Health (WSBOH) looks good on the surface but is incredibly misleading.
1. They use a relative risk reduction approach rather than an absolute risk reduction calculation.
2. The majority of the placebo group crosses over into the inoculated group, which means it’s no longer a randomized controlled trial.
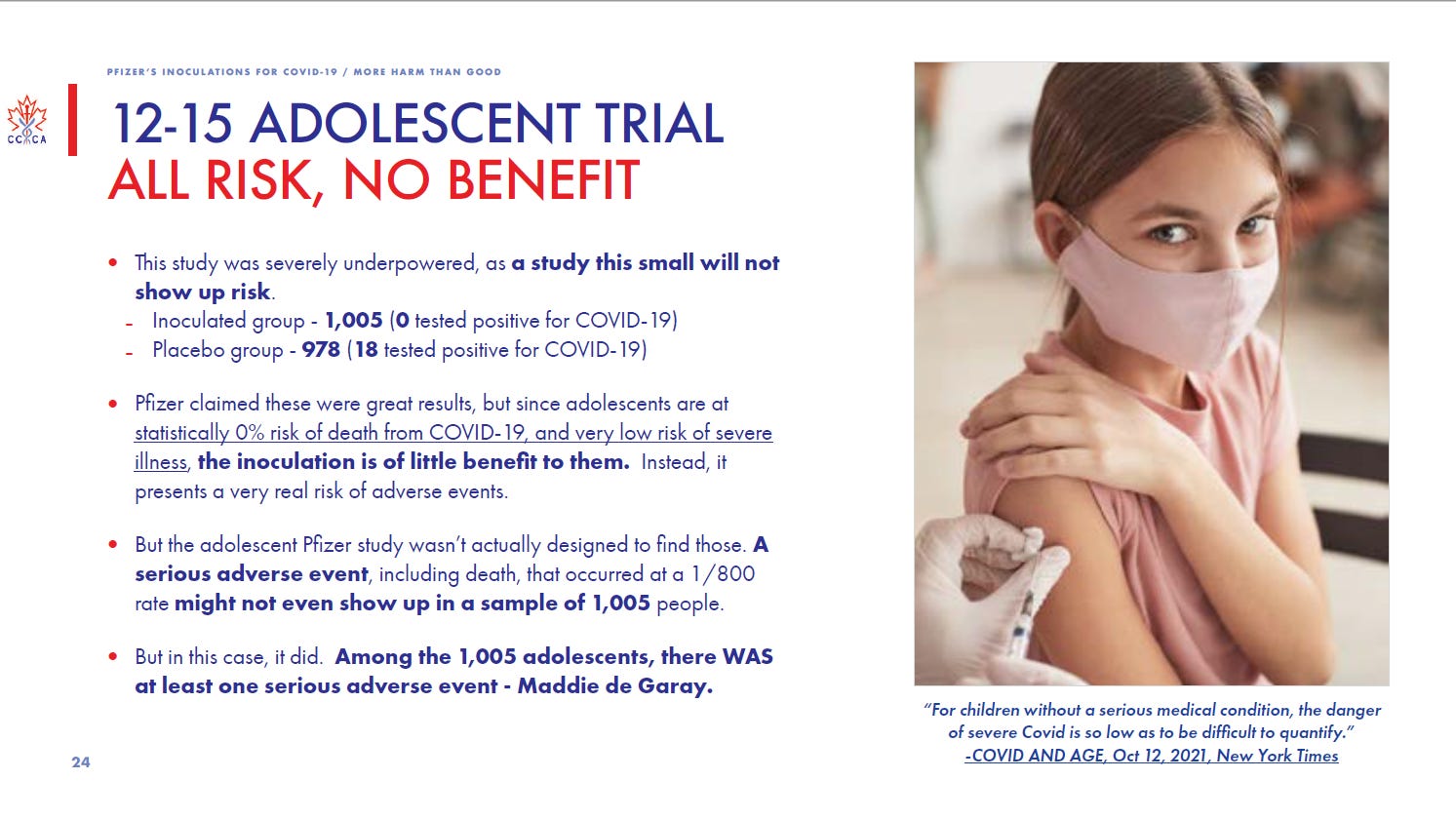
3. They do not use an unvaccinated control group, the control group is given another type of vaccine, again not a randomized controlled trial with a placebo. Below is an image of how they should have designed their control groups from the Canadian Covid Care Alliance.

4. They did not show the overall increase in illness and death in the COVID vaccinated treatment group.
5. The rates of severe COVID symptoms in children are so low their study design and test subject numbers are completely inadequate.
6. They did not test for disease biomarkers such as D dimer, C-reactive protein, troponins, occludin, claudin, blood oxygen levels, or for serum HMGB1, CXCL13, and Disckkopf-1 (markers for increased predisposition to autoimmune disease.)
7. Testing if the COVID-19 injections reduce the spread of disease and transmission was not studied as an endpoint. There is no evidence that they reduce the spread of the disease, especially in children.
8. The presented data was obtained with the RT-PCR test that is no longer recommended by the CDC because of the unacceptable rate of false positives and failure to determine contagiousness. There are different protocols for testing vaccinated and unvaccinated individuals with different cycle count thresholds to falsely elevate case numbers in the unvaccinated. In addition, unvaccinated adolescent athletes are subject to frequent testing again falsely elevating cases in the unvaccinated.
9. The Pfizer trials did not test all participants for COVID-19. This trial design subjectivity left it up to the investigator to decide whether to test and another reason for unreliable results.
10. Pfizer and the FDA have been battling in court to keep their safety data confidential for 55 and then 75 years. How can the TAG group make an educated decision regarding these experimental products without the proper safety data?
11. Without the proper studies, control group, and safety data there can be no informed consent.
12. How could the TAG even consider adding an experimental product to the vaccine schedule for school age children and those attending day care and preschool (3-5 years) when the FDA has not even approved an EUA for children under 5 years?
13. Why would the TAG approve criteria 5 without the proper evidence and criteria 6 with ALMOST NO EVIDENCE? To me it reeks of a compromised group of people who nobody elected and do not care about our children, informed consent, medical freedom, or civil rights.
I want to extend a sincere thank you for all of you who provided a comment or testimony to the WSBOH and/or to the FDA about the EUA for children under 5. Because of awesome people like you they are aware of our reservations as parents and people who care about children. I would also like to thank my friend who is working on a rebuttal to criteria 6 and all of the amazing writers on Substack!
References
- https://sboh.wa.gov/sites/default/files/2022-01/ImmunizationCriteria_a.pdf
- https://popularrationalism.substack.com/p/the-vaccine-lifecycle-lead-to-vaccine
- https://roundingtheearth.substack.com/p/vaccine-induced-mortality-part-8
- https://openvaers.com/covid-data
- https://jessicar.substack.com/p/there-are-25754-adverse-event-reports
- https://openvaers.com/covid-data/myo-pericarditis
- https://stevekirsch.substack.com/p/this-medical-data-from-the-us-dod
- https://rwmalonemd.substack.com/p/regarding-the-defense-medical-epidemiological
- https://health.mil/Military-Health-Topics/Combat-Support/Armed-Forces-Health-Surveillance-Division/Data-Management-and-Technical-Support/Defense-Medical-Surveillance-System
- https://stevekirsch.substack.com/p/unprecedented-deaths-in-indiana-for
- https://pubmed.ncbi.nlm.nih.gov/34664804/
- https://www.bitchute.com/video/93bc4eyNPFl5/
- https://report24.news/ab-13-jahren-lange-liste-ploetzlich-verstorbener-oder-schwerkranker-sportler/
- https://rwmalonemd.substack.com/p/a-health-public-policy-nightmare
- https://globalcovidsummit.org/news/live-stream-event-physicians-alerting-parents
- http://indepthnh.org/wp-content/uploads/2021/10/COVID-Report-from-Rep.-Weyler-3.pdf
- thecentersquare.com/indiana/indiana-life-insurance-ceo-says-deaths-are-up-40-among-people-ages-18-64/article_71473b12-6b1e-11ec-8641-5b2c06725e2c.html
- https://denisrancourt.ca/entries.php?id=109&name=2022_02_09_nature_of_the_toxicity_of_the_covid_19_vaccines_in_the_u
- https://zanaacarverphd.substack.com/p/whos-more-at-risk-from-the-c-19-injections
- https://stevekirsch.substack.com/p/bhakdiburkhardt-pathology-results
- https://doctors4covidethics.org/wp-content/uploads/2021/12/end-covax.pdf
- https://www.canadiancovidcarealliance.org/
- https://www.canadiancovidcarealliance.org/wp-content/uploads/2022/02/Scientific-Review-Dispelling-the-Myth-of-a-Pandemic-of-the-Unvaccinated.pdf
- https://www.canadiancovidcarealliance.org/wp-content/uploads/2021/12/The-COVID-19-Inoculations-More-Harm-Than-Good-REV-Dec-16-2021.pdf